
Shared Decision Making
In an era where there are so many options in the medical field, having the opportunity for shared decision making is more important than ever. Shared decision making is when a doctor and patient decide together on what needs to be done next. This contrasts with the more traditional practice of medicine in the 19th and 20th centuries, where the health care providers had the knowledge and dictated to the patients and their families of what needed to be done. Shared decision making is important when more than one option is being presented and it’s not 100% clear on what needs to be done. In a more “clear cut” situation, the role of shared decision making is less pronounced. For example, a young person comes in with acute appendicitis. We know that if we don’t operate and remove the appendix quickly, it can burst, cause peritonitis and ultimately lead to death. We wouldn’t converse about it for an hour with the patient and his family; we would say that this is what needs to be done and this is what we are going to do. Another common case (that I have often experienced as a cardiologist) is when someone is having a heart attack. We know that it’s important to move quickly and take care of the situation, and giving a variety of options is not the best use of time.

In instances that have more than one option and are not as acute (or urgent), shared decision making is a very ethical option and practice with most physicians. Here’s an example of how this tends to play out: say we have a patient who comes in for an appointment. She feels fine, and has no symptoms of an impending heart attack or stroke, but is considered high risk. As a doctor, I offer the option of prescribing a statin (which lowers cholesterol). These medications have been widely used since the 1980s and have been credited for cutting the number of heart attacks in half. They have been very powerful and useful, but they need to be taken on a daily basis. While they are generally safe to use, it’s important to remember that there are no medications without side effects. Statins are not “muscle friendly”, and approximately 1 in 5 patients develops muscle aches while taking this medication. This is not life-threatening, but it can inhibit daily activities. It becomes a back and forth discussion that takes time and effort from both the patient and the doctor. Of course, it is much easier for a doctor to say “here is your prescription, take this daily and come back in two months so I can check your cholesterol levels”. But the approach where the physician invites the patient to make decisions together based on the patient’s comfort level can be extremely beneficial. On one hand, we want to educate the patient on what we think is best; but on the other hand, we want him to be able to follow through with that decision.
Shared decision making is a wonderful thing. It’s what patients deserve, but it takes time and a good attitude from both the patient and the physician. It takes the realization from the patient that there are no easy fixes in medicine and that prevention is the first line of defense. Does your doctor practice shared decision making? If you’re not sure, have a discussion with her and find what fits your needs the best.
To your health!
Dr. Anthony

Should we be taking aspirin daily to prevent heart attacks and strokes?
Aspirin is a medication we have been using for over one hundred years. At a low dose, which averages between 40-100 mg a day, aspirin has been used in the last two to three decades primarily for the prevention of heart attacks and strokes.

We know that heart attacks and strokes can occur when cholesterol plaque in one of our major heart or brain arteries first develops, then matures (which can take decades!), and -- without warning -- becomes unstable and cracks. When it reaches this point, the blood flow over the unstable plaque recognizes the situation as “bleeding” or a “hole” in the artery. It tries to repair the situation by flowing very quickly to where it believes the problem is happening, and in the process can form a clot over the unstable plaque in less than one minute. So here we have a situation where a cholesterol plaque may only obstruct 10-20% of the opening (lumen) of a heart or brain artery. When this plaque becomes unstable, the blood forms a clot over it and within a minute there is a 100% obstruction of the blood flow. Because there is no blood flow through the artery, the cells start dying in a matter of 3 minutes for the brain and 30 minutes for the heart. This is how most heart attacks and strokes can occur.
A low dose of aspirin works by inhibiting the sticky cells in the blood, called platelets, from sticking together and forming a clot. However, at a high dose, aspirin also inhibits various enzymes and good cells. While a low dose would protect the arteries from clotting, a higher dose would not. This is why we have been using a low dose for the prevention of heart attacks and strokes. If too much aspirin is taken, it can cause bleeding, which has the reverse effect and can encourage clotting of the arteries.
Those who have had a heart attack or stroke are instructed to continue taking a low dose of aspirin every day for the rest of their lives. However, we must remember that science has no “last word”: it’s all based on the function of time and the evaluation of the available evidence.
So let’s say that the evidence from twenty years ago overwhelmingly supported using aspirin for the prevention of heart attacks and strokes -- not only for secondary prevention (meaning you’ve already had a heart attack or stroke and you’re taking it as a way to prevent this from happening again), but for primary prevention, which means you never had a heart attack or stroke, but you were deemed to be at a higher risk for suffering from one. This includes people with diabetes, smokers, those with high LDL or high blood pressure, a family history of heart disease, etc. For all of these people, we thought it made sense to give a low dose every day for the rest of their lives to prevent heart attacks or strokes from ever occurring in the first place.
A few months ago, science came forward and said that this is not correct. We have reevaluated the evidence, and in the modern era of medicine-- with better use of “statins” (Lipitor, Crestor, etc), medications that lower the LDL (bad cholesterol), and improved treatment of high blood pressure-- we don’t think the benefits of taking aspirin for primary prevention outweigh the risks. This is big news for patients and doctors!
Randomized trials and observations from the American College of Cardiology and the American Heart Association, which included tens of thousands of patients for years, have concluded that the use of aspirin is no longer appropriate for primary prevention of heart attacks and strokes -- except for those at very high risk (meaning those who have at least a 10% risk of developing heart attacks or strokes over the next ten years). The studies indicated that patients who have already had a heart attack or stroke should absolutely continue taking aspirin for secondary prevention. But for using aspirin for primary prevention, we have to really dive into the risk factors of the patient (age, family history, lifestyle, blood pressure level, cholesterol level) and determine if this is appropriate. Only if we evaluate these factors as being high, and the risk of bleeding from aspirin is low, then it is ok to use aspirin for primary prevention.
As with any kind of medication or regimen, please speak with your doctor before determining whether you should start or stop taking aspirin.
To your health!
Dr. Anthony
New Year, New Diet? - Keto (Part 1 of 3)
A New Year! Another chance for us to start fresh and make the most out of the year. With the New Year comes resolutions -- and the most common one? To lose weight! While there are many different kinds of diets, exercises and ways to get healthy, in my book I discuss the positive health benefits of two trendy diets: the Paleo Diet and the Mediterranean Diet. I stand by these two ways - or philosophies - of eating more than any other kind of plan. However, I also need to acknowledge another diet that is making waves in the health industry: the Keto Diet.
The Keto Diet has become extremely popular -- and for a good reason, as it helps you lose a lot of weight in a relatively short amount of time and without feeling hungry. Keto diet, or “The Diet Without Carbs”, consists mainly of protein, fat, and vegetables. However, it’s a strict diet: can you imagine spending the rest of your life without ever again tasting fruits, bread, pasta, milk or ice cream?! So, if you are looking to try a new way of eating, read below as I give a little synopsis into these three popular diets! Let’s start with the Keto Diet.

The Keto diet is higher in fats and proteins, and keeps carbs down to a minimum.
The Ketogenic Diet, or Keto diet as it’s commonly referred to, has taken the country by storm. The Keto diet is based around the high consumption of fats, proteins, and vegetables while limiting carbohydrates to no more than 20 grams per day (think that even spinach contains 1 gm of sugar per serving). By eating foods that are higher in fat and protein, the body stays fuller longer and that’s the key secret of this diet: you don’t have to feel hungry to lose weight. The fats you can eat include both the heavy saturated fats like bacon, red meats, and excess cheeses, but also the healthier fat choices, like avocados, eggs, and coconut oils. The only carbs that are allowed in the Keto diet are those mainly those found in vegetables and berries. Carbs (such as simple sugars, high Glycemic Index foods, white bread, white pasta, and even some fruits) are extremely restricted as they force insulin to spike. This leads to mild hypoglycemia and hunger. Imagine that you eat to stay full and satisfied, instead of eating every 2 hours when hunger strikes -- which is what simple sugars do!
Beyond being so strict and so difficult to maintain over time, another drawback to trying the Keto diet is the Keto flu. This occurs because our brain is programmed to run on sugar. With the Keto diet, you take sugars out which forces the brain to make an unpleasant adjustment and run on fat instead. The brain doesn’t like that and will let you know: you can feel extremely tired, with possible constipation or diarrhea, as well as bloating. These symptoms may last anywhere from a few days to a few weeks -- but that is to be expected as our bodies get outside their comfort zone (or comfort food!) and have to go through such a drastic transition over such a short period of time. Most scientists do not like the Keto diet because it allows you to eat large quantities of saturated and bad fats. But the main problem that a lot of people deal with on the Keto diet is the inability to maintain the changes in the long run. If you have followed the Keto diet for an extended period of time, lost the desired amount of weight and then go back to your old ways of eating, the weight that you lost will come right back. So, can you stay away from beer, pasta, bread or milk chocolate forever? Not many people have done it.
Finally, I want to add that, as a doctor, I am frequently asked about what this kind of eating does to our arteries, mainly because of the consumption of high fats. The answer comes down to this: if you are obese or significantly overweight, losing the excess weight (in fat) is much healthier in the long run than the effects of a high-fat diet.
Stay tuned! I will discuss two other tasty diets that you can adhere to in the long run and are approved by many scientists.
To your health!
Dr. Anthony
Know someone who would appreciate this blog? Share it with them!
The Tip of the Iceberg
Last week I was honored to present on the obesity-diabetes-and artery disease epidemic to a group of Delta employees in Atlanta. The venue was warm and inviting and very well organized. The participants were engaged and asked a large number of insightful questions. After my talk was over, I was invited to one of the working areas and I was happy to see that there were so many standing desks and a lot of opportunities for the employees to be physically active. A great workplace!
I used several PowerPoint slides for my presentation. One of those showed a picture of a gigantic iceberg where both the above-the-surface and below-the-surface parts of the iceberg were visible. The caption read: “Why am I showing you this picture?” After I let the question sink in the minds of the audience for a few seconds, I presented the next slide. There was the picture of a huge belly of a man. The face or the rest of the body were not shown; the focus was on the belly. The caption read: “Because it is so easy to see this…”. The next slide followed in quick succession and its caption picked up where the previous one left: “...but you can’t see that!”
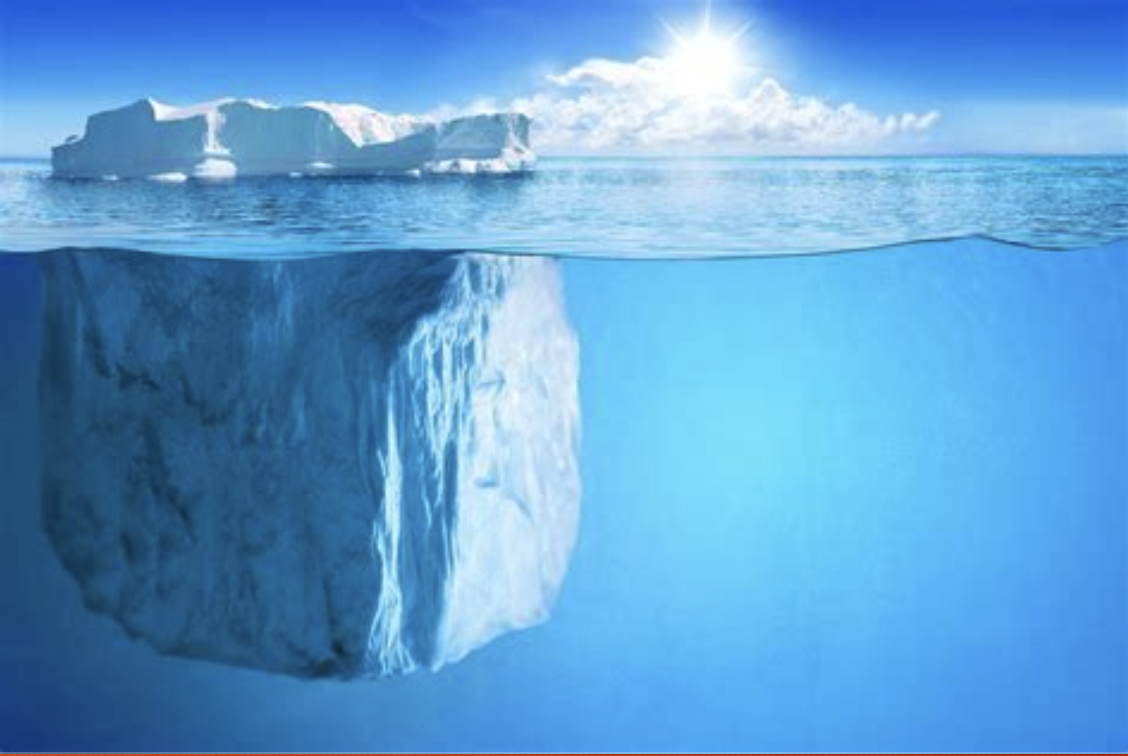

Just like the iceberg that sunk the Titanic, what is hiding below the surface is the most dangerous. Our artery health can’t be seen from the outside, but inside, the story is much different.

You can clearly see the “deeper issue” in this up-close photo of an adult artery.
The “that” was the inside of an artery of a person with a huge belly like the one on the slide. The artery looked ugly, like a war zone. Instead of appearing like a smooth glistening tube, the inside of the artery was uneven, filled with dirty-looking red and yellow growths, like tumors. These tumors were not cancers; they were advanced-stage cholesterol plaques with bleeding and clots on their surface. Such an artery can become the cause of a heart attack, stroke or sudden death without further notice. The slide that followed showed exactly how such a thing can happen. Most of us (especially men) start developing thin fatty lines in the wall of our arteries when we are teenagers. These early fat accumulations are called “fatty streaks” and represent the only form of cholesterol accumulation in our arteries that is reversible. As the cholesterol plaques continue to develop, it usually takes them a minimum of 20 plus years to mature and, usually, cause zero symptoms during that phase. Once mature, they can, all of a sudden and without any further warning, become unstable, and within a minute they can be causing serious symptoms like chest pain, heart attack, stroke or even sudden death.
Unfortunately, in western countries like ours, by the time we are 45 years of age most of us (especially men) do have some cholesterol plaque in the walls of our arteries. As long as these plaques stay stable, they are not a health problem and usually cause no symptoms. Once unstable, the result is catastrophic. So, what do we need to do to keep any plaques stable:
No smoking (not even one or two cigarettes a day)
Keeping our blood pressure and LDL cholesterol low (our health care provider will advise us whether or not we need medications to achieve this)
Staying physically and socially active
Eating a healthy diet with an emphasis on avoiding abdominal obesity by excluding fast carbs
Avoiding alcohol abuse
Sleeping at least 7 hours per night
Avoiding excessive stress
So, take good care of your arteries in order to keep any possible cholesterol plaques at bay and enjoy a long life without heart attacks, strokes or the need for heart surgery or other heart procedures.
To your health,
Dr. Anthony

Please HELP! What do I do about my Belly Fat?

Excessive belly fat (a waistline over 40 inches in men or over 35 inches in women) can destroy your metabolism and damage your arteries. It is also an early sign that you may be on your way to becoming diabetic, developing high blood pressure and, later, heart attacks or stroke. It also increases your chances of colon and breast cancer and Alzheimer’s disease. So what do you do?
Given the importance of belly fat, it is natural for people to try to get more information by googling it. If you google “belly fat” you may be directed to websites with advertisement for pills, supplements, shakes and drinks that “guarantee” you will lose belly fat. Should you believe them? Like most health-related issues, there are no easy fixes for abdobesity (excess belly fat); if they existed there would have not been as many people with a big belly walking around. But, in order to be fair about the web, one can find credible sites from reputable hospitals like Cleveland and Mayo Clinic, professional medical organizations like the American Diabetes Association and the American Heart Association or recommendations from professionals like physicians, registered nurses, registered dieticians or exercise physiologists. None of these credible websites will ever claim that you can lose your excess belly fat in a few weeks and keep it off for the rest of your life with a minimum effort.
In my book Abdobesity, I explain the seriousness of the belly fat and show how it is damaging our body’s metabolism and arteries’ health. As opposed to fat under the skin or around our hips (which is metabolically innocent), belly fat is directly wired to the liver, our chief metabolic factory. Under the constant negative influence of the belly fat, our liver is turned into a production line of chemical poisons that induce inflammation all over our body and promote cholesterol plaque development in our arteries; along with the other risk factors (smoking, high blood pressure, high LDL, diabetes, aging and family history) these cholesterol artery plaques mature overtime and they may become unstable as unpredictably as an earthquake. If this happens a heart attack, a stroke or sudden death follow with little or no warning. This is why a healthy lifestyle and early and aggressive treatment (with medications, if necessary) of high blood pressure, high LDL cholesterol or diabetes are so important; to effectively protect our artery health, however, they must be implemented as early in life as possible.
Don’t let abdobesity (excess belly fat) and the catastrophes that may follow it irreversibly damage your health and ruin your life. Espouse the elements of a healthy lifestyle; monitor your blood pressure, blood sugar and cholesterol; and nurture a close relationship with your primary care physician. Start by measuring your waist; if your numbers are in the red, don’t wait; take action. And, if you ever find your daily battle against abdobesity difficult or impossible, think of those who need you and believe in you: how will they be affected if your health takes a turn for the worse?
To your health!
Dr. Anthony